Clitoral Restoration
Welcome to Legacy Surgical Partners – we look forward to caring for you! Our priority is to make your surgery process and everything in between as pleasurable, empowering, and accessible as possible. Patients are expected to follow guidelines established by the WPATH Standards of care Version 8. We follow these standards—not as a gatekeeping hurdle—but as minimal guidelines that are useful guideposts that are protective. Though regret for gender affirming surgery is extremely rare, we are medical professionals who are here at your bequest. Surgery is irreversible, which puts the onus of responsibility on both patient and provider.
We're here to help you make essential decisions and know what to expect in surgery planning and recovery. Our team consists of:
- Surgeons
- A physician assistant
- Medical assistants
- Our surgery scheduler
- Office team
- And you
That's right, you! We value your input, your perspective and all the work you are and will be doing to prepare for and recover from surgery. We look forward to getting to know you better and learning how we can help you.
We want to make your surgery and recovery as smooth as possible. We’ll answer any questions you have and make sure you have the best possible outcome.
I. History
Dr. Bowers is one of very few surgeons worldwide who perform surgical reversal of Female Genital Mutilation/cutting (FGM/c). In 2007 and 2009, Dr. Bowers traveled to France and was the first surgeon to receive instruction from pioneering urologic surgeon, Dr. Pierre Foldès.1,2 Utilizing Foldès' acquired surgical techniques, Dr. Bowers removes scar tissue, corrects and reverses infibulation, and mobilizes the sensory clitoral body in order to restore clitoral sensation. She performs these surgeries at no cost to patients (although there is an operating room and anesthesia fee). The surgical procedure is conceptually simple but complex in the variety of anatomical challenges with FGM and its anatomical subtypes. The surgical procedure is short in duration (under one hour) under full anesthesia with most patients experiencing improved cosmetic appearance, sensation, and reduction in pain. Many are able to achieve orgasm following clitoral restoration.3
Although there are numerous clinical affirmations and studies which suggest efficacy of Clitoral Restoration, there are few studies that evaluate outcomes nor any that utilize standard measures of sexual function (FSFI). The best study remains Foldès' landmark paper in 2012 in which nearly 2,938 FGM survivors with FGM types II or III were followed prospectively after undergoing restorative surgery. To summarize, 99% were glad they underwent surgery, 80% reported improved sexual function, and more than 50% were able to achieve orgasm, many for the first time.3
In March of 2014, Dr. Bowers traveled to Africa to train surgeons at the Hospital Kamkaso "Pleasure Hospital" in Burkina Faso, but were rebuffed by governmental restrictions, Al-Qaeda incursions in 2015, and 2 coups d'état. Her hospital, expressly devoted to the care of FGM/c survivors, L'Hôpital Komkaso, was built but never opened.4
Recognizing her limitations as the sole surgeon performing Foldès-type clitoral restoration in the US—primarily for immigrants to the US—Dr. Bowers sought to export surgical training to young surgeons in Africa. Partnering with gracious host and plastic surgeon, Dr. Adan Abdullahi, Dr. Bowers and her surgical team and support staff have been traveling to Nairobi, Kenya to perform restorative surgeries since 2017.4,5
For women considering Clitoral Restoration, there are many considerations. We attempt to be culturally respectful but disapproving of the cultural practices that lead to FGM. There appears to be a current of resistance against FGM in Africa with larger cities, countries (Kenya in 2011), and individuals beginning to say no to the practice.6 As women (and men!) communicate about the devastating effects on intimacy, relationships, and health due to FGM, the tide seems to be turning. Much of this education is leading to growing awareness of the consequences, that these so-called 'purifying' rituals do harm rather than good. Communication via cellphone and internet is helping to spread truth about this practice. That there is also a surgical procedure which can help to reverse FGM is also empowering to the people of Africa. News of successful outcomes in Kenya have spurred interest by outside doctors. In 2024, our first surgeon-trainee from Mogadishu, Somalia was brought to our surgical summit in Nairobi. Our goal in bringing the surgical procedure to Africa is to allow women to control their own destiny, to regain their sense of identity as women and as sexual human beings. Four additional surgeons are expected to join the 2026 mission.
Unfortunately, there remains enormous work to do. Even Burkina Faso, which has had wide support for the FGM reversal procedure and outlawed the practice of FGM in 1996, there are still pockets of stubbornness and misinformation which continue to support the cultural practice of FGM—as evidenced by our Burkinabè hospital denial and medical privilege revocation in 2014.7 Female sexuality is still devalued and traditions remain strong. A major source of perpetuation of the FGM practice are the towns and villages where the majority of Africans live. It is in these small villages where information can be manipulated and myths perpetuated. Unfortunately, it is often the 'cutters', women who benefit economically from performing FGM, who continue to promote FGM as 'beneficial' to young women and girls. These false claims of efficacy for FGM/C vary wildly from desirability to purification to improved health—all false and misleading. Quite the contrary, as women after FGM grow to have medical and obstetrical complications, urinary tract infections, indifference to sex and intimacy resulting in ruined relationships—due to FGM. Education, honesty and persistence are the keys to bringing a better future to the women of Africa. It is the People of Africa who will assume control of their collective futures.
Clitoral Restoration Surgery itself is generally considered successful. When Dr. Foldès, the procedure's inventor, published his data in The Lancet, skeptics emerged, particularly British gynecologists, who scoffed at Foldès' technique as theoretically impossible—without witnessing the procedure or considering the outcomes claimed. The fact is, if you listen to the account of even one woman reporting her awakened sensation and experiencing orgasm for the very first time in her life after FGM reversal, skepticism is no longer warranted. Exposure of the clitoral body allows the shortened nerves to be contacted tactilely. As regards the anatomy itself, the clitoris is much larger than described by lay persons. In reality, FGM/c itself removes less than 3% of the clitoris, primarily the glans but also the labia and clitoral hood. Clitoral Restoration Surgery uncovers what is remaining but, crucially, mobilizes the clitoral body forward and lower—so that it can be contacted sexually, if desired. Literally, removal of the tip of the iceberg does not rid the iceberg itself. We ALWAYS find the clitoral body during reversal procedures. Exposing, mobilizing and securing the clitoral body to the skin surface is the delicate and slightly complicated aspect of the procedure. Nearly 30% of CRS surgeries expose the intact clitoral glans.
Sources
- MarciBowers.com – FGM/C History
- Prolongeau H, Levin T. Undoing FGM: Pierre Foldès, the Surgeon Who Restores the Clitoris. UnCUT/VOICES Press, 2011.
- Foldès P, Cuzin B, Andro A. Reconstructive surgery after female genital mutilation: a prospective cohort study. The Lancet. 2012 Jul 14;380(9837):134-41.
- Marci Foundation – Our History
- The Standard Kenya – Restoring dignity of FGM survivors through surgery (December 2022)
- Kenya Law – Prohibition of Female Genital Mutilation Act No. 32 of 2011
- Future Policy – Burkina Faso: Law Prohibiting Female Genital Mutilation/Cutting (Law No.43/96/ADP of 1996)
II. Featured Articles

















III. Resources
IV. Surgical Results Gallery
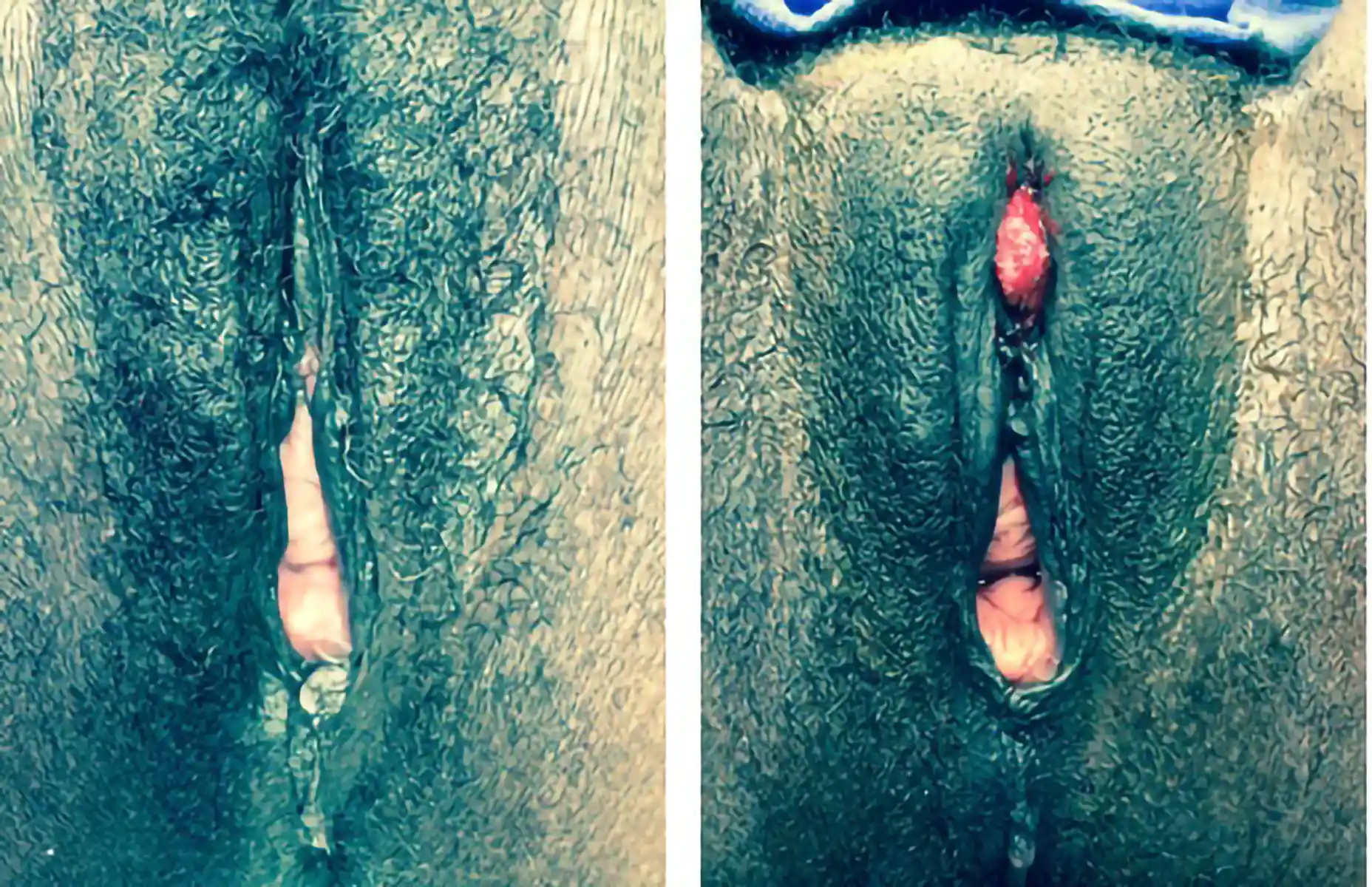
Below are examples of real Clitoral Restoration surgeries performed by our team. These images are shared with full patient consent and are intended to help you understand what to expect. They include pre-op and post-op views, which may contain nudity and surgical results.

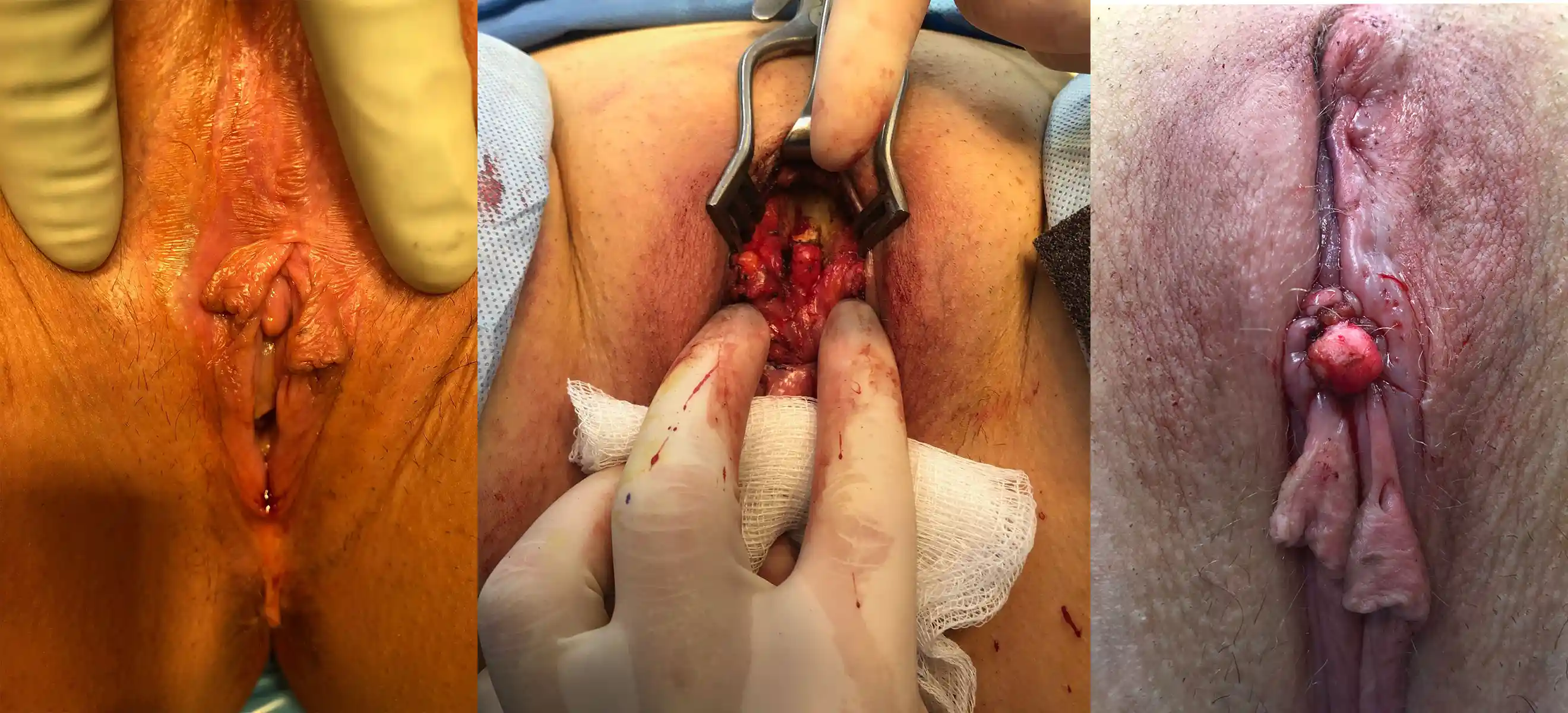






![Type III FGM case showing [top left] preoperative, [top right] immediate postoperative, and [second row] three-week postoperative stages, demonstrating progressive restoration and healing.](https://cdn.prod.website-files.com/693cb6ff51584191bed8f2c2/693cb6ff51584191bed8f5db_uc.webp)